
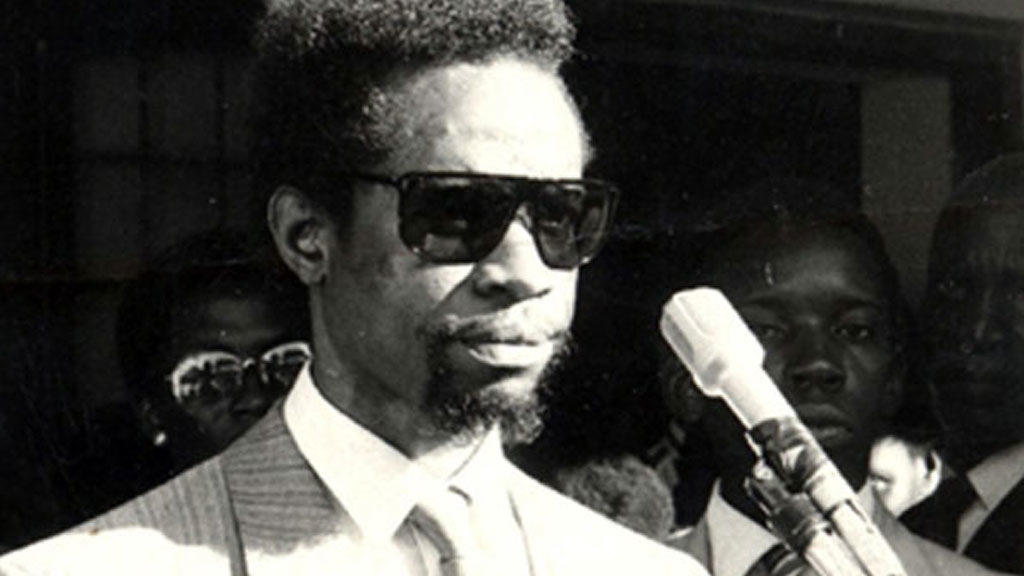
It was on April 18th 1989, Philly Bongoley Lutaaya, a prominent Ugandan musician, made a groundbreaking announcement became the first prominent African to announce: he revealed that he was HIV-positive. At the time, HIV/AIDS was heavily stigmatized in Uganda, often referred to as “Silimu” (meaning “slim”) due to the severe weight loss it caused in victims. Diagnosed in 1989 at the peak of his career, Lutaaya became the first high-profile Ugandan to publicly disclose his HIV status, a bold move in an era of fear and misinformation about the disease.

His decision to go public earned him global praise, but it also unintentionally exposed his children to stigma and discrimination. By sharing his status, Lutaaya humanized the epidemic, challenging the perception that HIV/AIDS only affected marginalized communities. He showed that even a celebrated urban figure like himself could be vulnerable to the same struggles as someone in a rural village. When he discussed his decision with his family, his brother initially opposed it, fearing the harsh treatment HIV patients faced, including being ostracized and secluded from their families.
Despite the backlash, Philly remained steadfast. At the dawn of the year 1989, he announced his diagnosis to the students at a press conference in Makerere University Kampala, but many doubted him because he appeared healthy and had just released a successful album, Born in Africa. Some even accused him of fabricating the story to boost his music sales. Undeterred, Philly continued to speak out, determined to raise awareness about the crisis.
As his health declined, Philly sent his children to live with foster families in Sweden, shielding them from the reality of his illness and the discrimination that was already setting in from the public. He also returned to Sweden for treatment, with visible signs of AIDS and diffuse disease. He was even unable to stand due to the sores on his feet, but was always hopeful and a lover of life. There as he received his treatment, recorded his album; Alone and Frightened, in a bid to spread the message om HIV/AIDS and realities of the stigma he faced coming out to openly announce his status. He fought tooth and nail and sought all the necessary treatment to see that he stood on his own two feet and get the strength he needed to return to Uganda to release his album and spread the word about the reality of the disease. He had an American crew that was filming his time and the message that he intended to put across, and it was stopped by Ugandan government because of the negative face Uganda was getting in the international eye as a hub for HIV/AIDS. However he urged them that it was his dying wish to spread awareness and bring light to the matter, and so they eventually let up.

After the album’s release, he spread awareness to schools, churches, communities and many others. He provided mentorship to people living with HIV Ugandans at TAASO and even to those not affiliated with it, which gave them hope and encouragement. He took AIDS out of the textbook and put a face to it.
He returned to Sweden about a month later to continue his treatment and hold onto the little time he had left with his children. Feeling frail and life slipping away from him, he requested to be returned to Uganda shortly after, to accomplish his dying wish; to die in Africa which he held so dear to his heart; Born in Africa and Die in Africa. On December 15, 1989, Philly passed away shortly after his 38th birthday, leaving behind a legacy as a courageous advocate who challenged prejudice and brought hope to those affected by HIV/AIDS. He was eager about living a happy and impactful, and not let fear of death overshadow his demeanor even though he confessed, “It is a painful experience to know that you will never achieve your dreams”. His story remains a powerful reminder of the importance of compassion and awareness in the face of stigma. His documentary depicting his life and legacy can readily be watched here.
As an aspiring healthcare provider, the issue of HIV is both intimate and deeply significant to me. HIV, or Human Immunodeficiency Virus, and AIDS, or Acquired Immunodeficiency Syndrome, remain among the most pressing global health challenges. HIV is primarily transmitted through unprotected sexual intercourse, blood transfusion, shared needles among illicit drug users, and from mother to child during childbirth or breastfeeding. Once inside the body, the virus targets the immune system, specifically CD4 T-cells, which are essential in defending against infections.
In the first month after infection, an individual may experience flu-like symptoms such as fever, fatigue, and body aches. These symptoms can easily be mistaken for malaria or other common illnesses but typically subside on their own, even without treatment. This marks the acute phase of infection, during which the virus rapidly multiplies and spreads throughout the body.
Following this initial phase, HIV enters a prolonged latent stage that can last up to eight years. During this period, the virus continues to replicate at lower levels, gradually destroying CD4 T-cells. Although the individual remains asymptomatic, they can still unknowingly transmit the virus to others. Over time, as more immune cells are lost, the body’s ability to fight infections steadily declines.
When the CD4 count drops significantly, the immune system becomes severely compromised, leading to the onset of AIDS—the most advanced stage of HIV infection. At this point, the body is no longer able to defend itself against common infections, making even minor illnesses potentially life-threatening. Individuals at this stage often experience rapid and severe weight loss, extreme fatigue, prolonged diarrhea, persistent fever, and recurrent infections such as tuberculosis. Additionally, they become highly vulnerable to opportunistic diseases, including certain types of cancers.

Unfortunately, many individuals only seek medical attention when symptoms become severe, often leading to a diagnosis at an advanced stage when significant damage has already occurred.
This piece takes a moment to reflect on how far Uganda has come in the fight against HIV and the stigma surrounding it, while also recognizing the profound influence of Philly Lutaaya’s efforts and the progress his advocacy has helped to achieve.
In the 1980s, Uganda was widely regarded as the country most affected by HIV/AIDS. The nation’s HIV story is believed to have begun in 1982, when a mysterious illness emerged in Rakai, a rural district near Lake Victoria. Fishermen and traders returning from their travels began experiencing unexplained fevers, rashes, and rapid weight loss. Soon, their spouses fell ill, and entire families perished. By the late 1980s, the epidemic had spiraled out of control, with HIV prevalence soaring to 18% in rural areas and an alarming 30% in cities like Kampala. At the time, there was no government funding for condom distribution, and the virus spared no one. Teachers, soldiers, mothers, and children succumbed to the disease in overwhelming numbers—women being among the most affected. Ugandan musician Philly Lutaaya became the first African public figure to speak openly about living with HIV in 1989, helping to break the silence and stigma surrounding the disease.
Fortunately, Uganda’s relentless efforts in prevention, treatment, and awareness have led to remarkable progress. As of 2022, the national HIV prevalence has dropped to 5.1%, with a 40% reduction in new infections since 2010 and a 65% decrease in AIDS-related deaths. However, women continue to be disproportionately affected by the epidemic. Today, 1.4 million Ugandans live with HIV—not as victims, but as survivors. Their resilience stands as a testament to Uganda’s progress in fighting the epidemic and ensuring that those affected receive the care and support they need.
In terms of attitudes toward HIV, the disease has long been feared due to the absence of a known cure. Despite ongoing research efforts that have persisted for years, the fear of HIV remains pervasive. Ironically, risky sexual behavior continues to be a significant challenge to address. During the time of Philly Lutaaya, AIDS was perceived as a distant issue, primarily affecting the elderly; however, it has become increasingly evident that the prevalence of HIV is now a pressing concern among the youth, with rates 4% higher in females and 2% higher in males aged 15-49.
Philly’s message was clear: HIV is not just a disease of the impoverished, commercial sex workers, or marginalized communities; it can affect anyone, from the affluent to the poor, and from the young to the old. While stigma surrounding HIV has diminished somewhat over the years, it still lingers like a shadow. The association of HIV/AIDS with immorality remains strong, especially in a country where morals and religious values are held in high esteem, as evidenced by the national motto, “For God and my Country.” Consequently, openly disclosing one’s HIV status is often met with fear of judgment and social ostracism. In late 1989, shortly before his passing, Philly Lutaaya addressed an international women’s health conference, emphasizing the importance of shifting our focus in the battle against AIDS away from blame. He stated, “When we talk about the battle against AIDS, we must forget blame; blame is not productive. I know that I contracted the virus from a woman; but I don’t blame that woman. That woman was definitely given that virus by a man.”
Various reports from interactions with various African cultures have even framed HIV/AIDS as a form of divine punishment. The stigma does not end with the individual; it often extends to their families, who may continue to bear the burden of shame long after a loved one has passed. Gossip about the circumstances of their death can further compound this stigma. The stigma surrounding HIV causes many people living with the virus (PLHIV) to fear disclosing their status. As a result, they may withdraw from essential counseling services, delay the initiation of antiretroviral therapy (ART), and struggle to adopt safe practices.
Even within the healthcare system, stigma remains a challenge, as seen in Philly Lutaaya’s experience when he was turned away by two Ugandan doctors while seeking physiotherapy during his battle with the disease. However, the healthcare sector has since made significant strides in addressing this issue through various initiatives, which will be discussed ahead.
One key strategy has been the adoption of conscious and sensitive language in medical settings. For example, the term ‘people living with HIV’ (PLHIV) is now preferred over stigmatizing labels such as ‘HIV patients’ or ‘HIV-positive person,’ reinforcing the dignity and humanity of those affected. Additionally, some HIV clinics are intentionally not labeled as such or are strategically located in more discreet areas within hospitals to protect patient privacy. Medical records also use coded acronyms instead of explicitly stating a patient’s HIV status, further reducing the risk of stigma and discrimination. Despite these improvements, some healthcare personnel, due to ignorance or misinformation, still exhibit hesitation in directly engaging with PLHIV, highlighting the need for continued education and awareness within the sector.
Established in 1987, The AIDS Support Organization (TASO) began as a small group of volunteers dedicated to supporting individuals affected by HIV/AIDS amidst significant societal backlash and limited resources. Despite these challenges, TASO has grown into one of Uganda’s leading HIV/AIDS service organizations. A cornerstone of its approach is the training of HIV-positive “expert clients” who mentor and support others living with the virus. These expert clients provide peer-based guidance, helping to navigate the complexities of treatment and fostering a sense of community. Through initiatives like this, TASO continues to combat stigma and enhance the quality of life for people living with HIV in Uganda.

Uganda’s significant decline in HIV prevalence is the result of multifaceted strategies and unwavering commitment. The ABC campaign—Abstinence, Be Faithful, and Condom Use—emerged as a pioneering model across Africa and internationally studied, promoting behavioral changes that have been instrumental in reducing infection rates. Under President Museveni’s leadership, the government took a proactive approach to tackling the crisis, launching grassroots education programs in schools, markets, and places of worship. I can still vividly recall memorizing the ABC strategy alongside HIV/AIDS education at a young age during my early primary school years—it was ingrained in our education from the very start. This comprehensive approach fostered widespread awareness and community involvement. Religious leaders, who had previously remained silent, began advocating for compassion and understanding, further diminishing stigma and encouraging open dialogue even in places of worship.

In its ongoing efforts to combat the epidemic, Uganda also implemented a National Strategic Plan (NSP) encompassing four key pillars: Prevention; Care and Treatment; Social Support and Protection; and Systems Strengthening. A critical component of this plan is the concerted effort to eliminate stigma and discrimination against people living with HIV (PLHIV) and other vulnerable groups within communities and healthcare settings.
The government’s resolve has been pivotal in these advancements. In 2016, Uganda adopted the World Health Organization’s “Test-and-Treat” policy, ensuring that all HIV-positive individuals receive antiretroviral therapy (ART) regardless of their CD4 count. This policy shift has been complemented by the dedication of over 180,000 Village Health Team (VHT) volunteers, who traverse remote areas equipped with testing kits and medications, ensuring that even the most isolated communities have access to care. Innovations such as boda-boda (motorcycle) ambulances have been introduced to deliver ART to hard-to-reach locations, including islands and refugee settlements. Since 2020, Pre-Exposure Prophylaxis (PrEP) has been made freely available to high-risk groups, including sex workers, truck drivers, and discordant couples, offering an additional layer of protection against the virus.
Moreover, Uganda has enacted policies to safeguard PLHIV from discrimination in employment and education sectors, fostering an environment of inclusivity and support. These comprehensive efforts underscore Uganda’s commitment to eradicating HIV/AIDS and improving the quality of life for all its citizens.
International support has also played a crucial role. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) and USAID have collectively invested billions into testing, treatment, and prevention initiatives, funding a substantial portion of Uganda’s HIV programs. By 2010, these contributions accounted for 85% of the country’s HIV-related funding, significantly bolstering the national response. USAID has played a pivotal role in Uganda’s fight against HIV/AIDS, making significant contributions over the years. Since 2004, it has funded the distribution of 200 million condoms annually, trained 50,000 healthcare workers, and provided life-saving antiretroviral therapy (ART) to 1.2 million Ugandans. Beyond medical interventions, its support extended to vulnerable populations, with 500,000 orphans receiving school grants—offering them a chance to break free from cycles of poverty and despair.
However, the abrupt suspension of USAID funding has thrown Uganda’s HIV/AIDS response into crisis, severely disrupting treatment and support services. Thousands of patients now find themselves without reliable access to medication, while the closure of standalone HIV clinics has forced many to seek care at general hospitals. This shift has raised serious concerns about stigma, confidentiality, and overcrowding. Essential services such as viral load monitoring, tuberculosis screening, and counseling have also been affected, making it increasingly difficult to ensure effective treatment and follow-up care.
The strain on healthcare facilities is becoming more pronounced. At clinics like Kamwokya Community Clinic, medication refills are now limited to just twice a week, further restricting access to life-saving drugs. Peer support systems—once a crucial pillar of HIV care—have collapsed, leaving many people living with HIV (PLHIV) feeling abandoned and isolated. Meanwhile, overwhelmed government hospitals, struggling to meet the growing demand, have begun charging consultation fees. Medication shortages have further compounded the crisis, with healthcare workers resorting to prescribing incomplete doses or incorrect drug combinations—heightening the risk of drug resistance.
With treatment access dwindling, many patients have been forced into desperate measures. Some are rationing their medication, taking ARVs every other day, while others are sharing their doses with family members. This not only weakens individual immune systems but also accelerates the emergence of drug-resistant HIV strains, threatening public health on a larger scale. At the same time, some private healthcare facilities have taken advantage of the crisis, dramatically increasing the prices of ARVs, making them unaffordable for low-income patients.
The government’s response has been sluggish, drawing sharp criticism from activists. While the Uganda AIDS Commission has scheduled a parliamentary discussion on the crisis, for many patients, the damage is already being felt. Without immediate intervention, Uganda faces a worsening HIV epidemic, with rising transmission rates, increased treatment failures, and deteriorating health outcomes for those affected. As uncertainty looms, people living with HIV/AIDS in Uganda find themselves in one of the most precarious moments in recent history, with their futures hanging in the balance.
In 1989, Philly Lutaaya stood alone. Today, we stand together. Let his courage remind us: The fight against HIV is a fight for our shared humanity. When we talk of Philly, we talk of hope—a hope that refuses to die, even in the face of death, and we continue to celebrate him Nationally every 17th October. His voice, once solitary, now echoes in clinics, schools, and the hearts of those who dare to believe that AIDS can be beaten. The road is long, but as long as we walk it together, no one need ever be alone again.

Leave a Reply